")

Early intervention and long-term effects
Differences to the natural body’s labor
In emergency situations, inducing labor and monitoring the birth process might be necessary and can save the life of the unborn.
In daily hospital routines, the majority of births will be induced for different reasons. Experience suggests that as soon as the initial medical exam renders the diagnosis of e.g. “uterine weakness”, the woman will receive labor-promoting medication. From then on, the labor contractions are no longer based on the common rhythm of mother and child, but are caused by a given dosage of medication, depending on the doctor’s assessment.
The natural contractions of the body usually increase slowly so that both, the mother and her child, have time to recover in between and prepare for the next wave. hormonal-orchestra-during-labour-and-birth.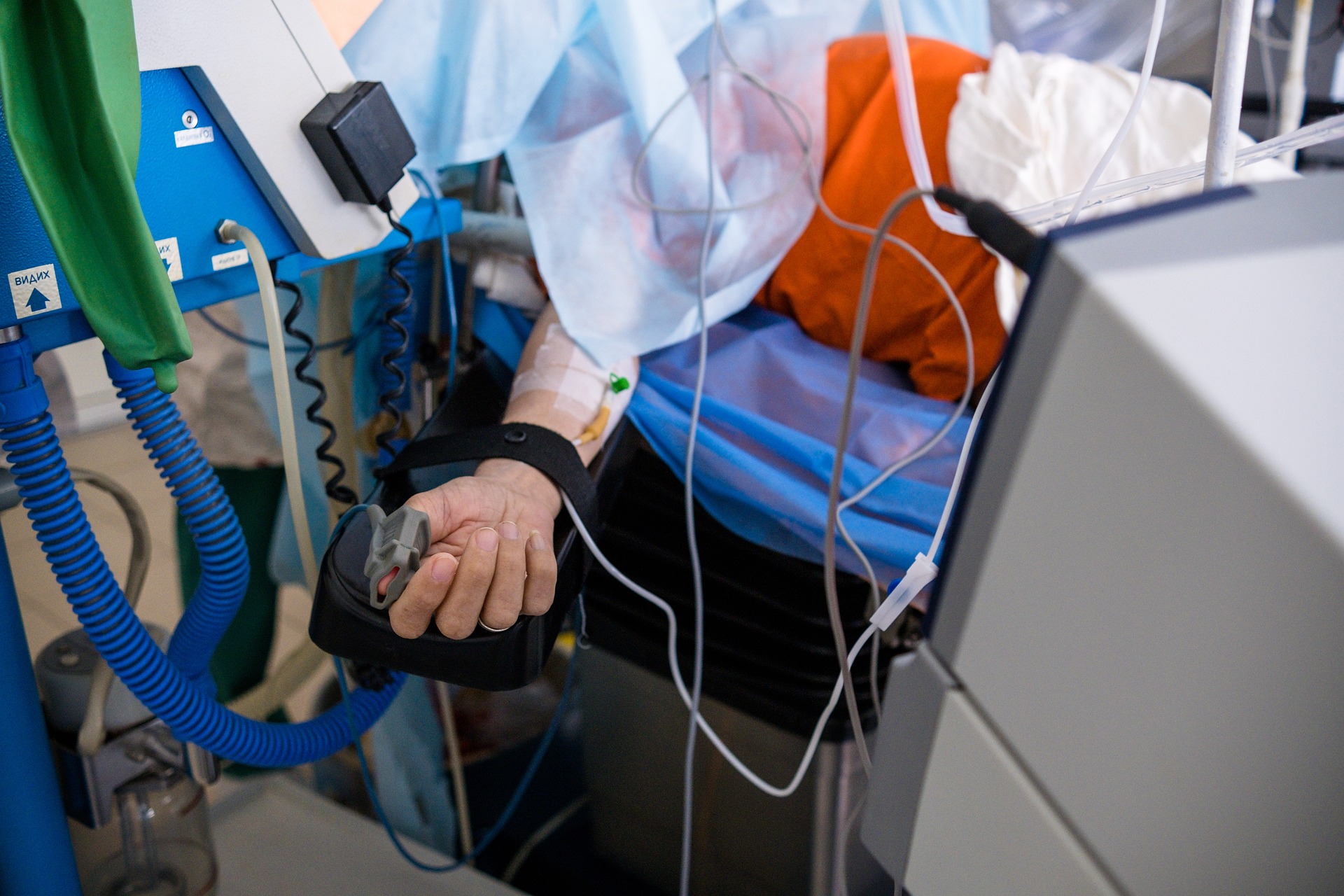 The pain caused by induced labor contractions, however, can build up too quickly, so that the mother cannot bear the pain and needs pain-reducing medication. This in turn can lower the mother’s blood pressure and, consequently, could reduce the blood circulation in the placenta. In order to prevent all of this from happening, the mother will receive stabilizing medication. Throughout the birthing process, the child’s heartbeat and the uterus contractions are monitored.
The pain caused by induced labor contractions, however, can build up too quickly, so that the mother cannot bear the pain and needs pain-reducing medication. This in turn can lower the mother’s blood pressure and, consequently, could reduce the blood circulation in the placenta. In order to prevent all of this from happening, the mother will receive stabilizing medication. Throughout the birthing process, the child’s heartbeat and the uterus contractions are monitored.
The most common diagnosis leading to a caesarean section is as follows: “faint heartbeat of the child”. Parents will always agree to this procedure for the sake of their child’s health. Most of the time they feel:” We are very fortunate that we are in the hospital.” They may not be aware of the fact that the side effects of already used medications, time pressure through shortage of medical staff, and lack of emotional support are very often the real reasons why a caesarean section is performed.
An involved mother describes the cascades of interventions as follows:
“I gave birth to my first daughter in a hospital in 2010, after 43 hours of labor. I received a Buscopan suppository (a spasmolytic), two Meptid infusions (an opioid analgesic), an epidural, an oxytocin drip (to promote uterine contractions), repeated drips with saline solutions, all the while being on an electronic fetal monitor (CTG). I had to go through countless painful vaginal exams by four different midwives and a senior female physician, periodic catheterizations, an unsolicited perineal incision, a Kristeller maneuver by yet another female doctor, the threat of a delivery through vacuum extraction (i.e. the vacuum device lay right there next to me ready to use), and finally a McRoberts maneuver because of shoulder dystocia. Most of the time I was left alone with my husband, helpless and scared, overwhelmed with the situation and the immense pain. The medical staff came only to provide medication, and was only present during the last hour before the actual birth.
I thought that births must happen in this way, and was even happy and grateful that a caesarean section was avoided, with which the doctors threatened me again and again.”